
When we hear the phrase ‘animal research’ we tend to think about the development of new drugs for the clinical practice, or studying molecular pathways involved in the progression of disease; but we must also remember that the techniques used in the operation room are a consequence of biomedical research, including the use of animals. It is not just the creation of these techniques but also for the prior steps necessary for us to consider a surgical technique as an option when faced with a disease. An example of this is research into a type of cancer known as Peritoneal Carcinosis (PC) and the development of a technique, known as HIPEC, that may dramatically improve the prognosis for patients with this type of cancer.
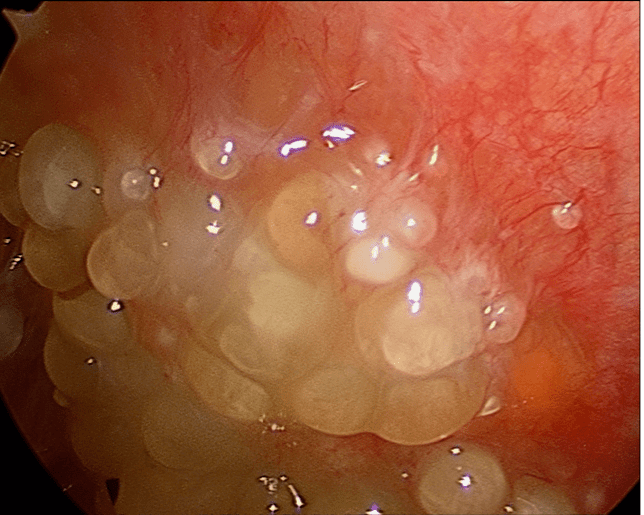
What is the definition of Peritoneal Carcinosis? We describe this medical condition as the presence of neoplastic nodules caused by the spreading of a primary or secondary tumor in the peritoneal cavity. The peritoneal cavity, also called the abdominal cavity, is the largest body cavity and contains many of the major organs – such as the liver, kidneys, stomach and intestines – surrounded by a protective membrane known as the peritoneum.
Although PC is sometimes seen in primary tumours, such as peritoneal mesothelioma or Pseudomyxoma peritoneii, it is more frequently observed as a metastatic diffusion of gastroenteric (stomach and colon, primary) or gynaecologic (ovarian) tumors. In the second situation, we could see it as an advanced manifestation present at the same time as the primary neoplastic disease or appearing in the years following treatment of the tumour. This condition is often associated with a poor prognosis (about 6 months), depending on the site to which it spreads, the involvement of abdominal organs (like colon or liver) and how aggressive is the tumor at the moment of diagnose.
In the past, physicians have had only two options when combating the disease: systemic chemotherapy or palliative surgical therapy to debulk the tumor masses- removing as much as possible of tumors which cannot be entirely removed – and prevent severe conditions such as bowel obstruction. Recently, surgical research developed another therapeutic approach, known as Cytoreduction (CR) associated with Hyperthermic intraperitoneal Chemotherapy (HIPEC). This technique consists of a two-part operation: during the first part, the surgeon debulks as much of the neoplastic nodules in the peritoneal cavity as possible, and in the second stage the peritoneal cavity is washed with a hyperthermic chemotherapy solution, where a solution containing a high concentration of chemotherapy drugs is heated to above body temperature (usually 41.5°-42.5°C) which increases absorption of the drugs by the target tumor and therefor their effectiveness.
The role of the hyperthermic solution and the possibility of using a high-dose of chemotherapic agent was developed through research in rodents and dogs: these studies demostrated that the peritoneal barrier itself is not a barrier that prevents substances from pass through it. This is in agreement with observations made during surgery in human patients, when we remove the peritoneum (for example, when we debulk a neoplastic nodule on a peritoneal surface with a technique known as peritonectomy) the rate at which drugs are cleared from peritoneal cavity is not significantly affected. [1]
Studies in dogs and subsequently in human volunteers demonstrated that the high concentration of chemotherapeutic drugs in the peritoneal cavity is not related to a high concentration of these in the blood stream [2]. In particular a key study undertaken in dogs by Rubin et al. [3], consisted of studying the effects of removing portions of the perotineum such as the the omentum, the mesentery or the small bowel on the clearance of substances like glucose, urea and insulin from the peritoneal cavity. Surprisingly, this experiment indicated that these operations do not influence the clearance of these substances. On the base of these observation, clinical studies were started on clearance of drugs from the peritoneal compartment:. These clinical studies demonstrated that the process observed in dog with other substances occured also with drugs and that, in some cases, the concentration of a drug within the peritoneal cavity could be extremely high without having effects on the concentration in the bloodstream.
A natural consequence of this evidence is that we can use a high-dose chemotherapy drug against these nodules without having systemic adverse effects on the patient, a problem frequently observed in conventional systemic chemotherapy. These studies also led researchers to reconsider the spreading of a tumour in the peritoneal cavity not as a systemic dissemination but as a local disease, and that treatment might be able to cure it rather than just have a palliative impact. If the peritoneal barrier can selectively allow only some molecules to pass through, it could have also an active role on slowing the diffusion of metastatic cancer cells.
This evidence, together with the property of hyperthermia in helping drugs to penetrate cancer cells [4], and avoid the normal defences that a tumor cell has, led to development of this ambitious surgical technique.
The results of this combined technique is clear. Against primary tumors this technique shows a high survival-rate after 5 years (reaching 96% in some studies [5]). Against secondary spreading of gastroenteric or gynaecological tumours it shows a lower efficacy that may be related to the more diverse biological characteristics of the tumor cells, to the physiopathological features (diffusion, tumor already treated with chemotherapy etc.) and also to the characteristics of the patient (such as clinical status, age, concomitant diseases) [6],[7],[8],[9]. The 5-years survival rate for PC from colorectal cancer, for example, according to studies conducted by Dr. Paul Sugarbaker of the Washington Cancer Institute, one of the most important researcher on this field, is around 40%, when the cytoreduction is complete and the disease is not so diffuse in the peritoneal cavity. [7] Also, this surgical approach can be uses a second time, in case of a recurrence of PC, and, ultimately, as a palliative treatment to delay complications and reduce suffering of the cancer patients.
These numbers could seem low but we have to consider that we’re facing a disease that is often fatal within six months if left untreated. This technique gives patients another chance until very recently, they did not have. Why? Because of research that was built up, in part, thanks to animal research
These results are a direct effect of research in the fields of surgery and oncology, from the including the development of more effective chemotherapic agents, research that, as we have said many times, requires the study of animals for everything from the basic understanding of the processes involved to the preclinical testing a new therapy’s effectiveness and safety profile.
Marco Delli Zotti
[1] Michael F. Flessner “The transport barrier in intraperitoneal therapy” Am J Physiol Renal Physiol 288:F433-F442, 2005. http://www.ncbi.nlm.nih.gov/pubmed/15692055
[2] Pierre Jacquet, Andrew Averbach, Arvil D. Stephens, O. Anthony Stuart, David Chang, Paul H. Sugarbaker “Heated Intraoperative Intraperitoneal Mitomycin C and Early Postoperative Intraperitoneal 5-Fluorouracil: Pharmacokinetic Studies” Oncology 1998;55:130–138 http://www.ncbi.nlm.nih.gov/pubmed/9499187
[3] Rubin J, Jones Q, Planch A, Rushton F, Bower J. “The importance of the abdominal viscera to pertioneal transport during peritoneal dialysis in the dog.” Am J Med Sciences 1986;292:203– 208. http://www.ncbi.nlm.nih.gov/pubmed/3752166
[4] Elwood P. Armour, Donna McEachern, Zhenhua Wang, et al. “Sensitivity of Human Cells to Mild Hyperthermia” Cancer Res 1993;53:2740-2744. http://www.ncbi.nlm.nih.gov/pubmed/8504414
[5] Yan TD, Black D, Savady R et al. “Systematic review on the efficacy of cytoreductive surgery and perioperative intraperitoneal chemotherapy for pseudomyxoma peritonei.” Ann Surg Oncol 2007;14:484-92 http://www.ncbi.nlm.nih.gov/pubmed/17054002
[6] Franco Roviello, Daniele Marrelli, Alessandro Neri, Daniela Cerretani, Giovanni de Manzoni, Corrado Pedrazzani, MD, Tommaso Cioppa, MD, Giacomo Nastri, MD, Giorgio Giorgi, Enrico Pinto
“Treatment of Peritoneal Carcinomatosis by Cytoreductive Surgery and Intraperitoneal Hyperthermic Chemoperfusion (IHCP): Postoperative Outcome and Risk Factors for Morbidity” World J Surg (2006) 30: 2033–2040 http://www.ncbi.nlm.nih.gov/pubmed/17006608
[7] Paul H. Sugarbaker “Review of a personal experience in the Management of Carcinomatosis and Sarcomatosis” Jpn J Clin Oncol 2001; 31(12)573-583 http://www.ncbi.nlm.nih.gov/pubmed/11902487
[8] Zanon C, Bortolini M, Chiappino I et al. “Cytoreductive surgery combined with intraperitoneal chemohyperthermia for the treatment of advanced colon cancer.” World J Surg. 2006 Nov;30(11):2025-32. http://www.ncbi.nlm.nih.gov/pubmed/17058031
[9] Bijelic L, Jonson A, Sugarbaker PH “Systematic review of cytoreductive surgery and heated intraoperative intraperitoneal chemotherapy for treatment of peritoneal carcinomatosis in primary and recurrent ovarian cancer.” Ann Oncol 2007;18:1943-50 http://www.ncbi.nlm.nih.gov/pubmed/17496308
To learn more about the role of animal research in advancing human and veterinary medicine, and the threat posed to this progress by the animal rights lobby, follow us on Facebook or Twitter.
