
by Jeremy D. Bailoo, PhD
In light of #WorldImmunizationWeek we are doing a series of posts which highlight facts pertaining to vaccine production, and how safety and efficacy is assessed (part 1). We also highlight the historical aspects that lead to the “anti-vaxxer” movement and why critical consideration of the facts pertaining to that movement is warranted (parts 2 and 3). Finally, we highlight some of the longer term repercussions of not pushing back against such misinformation as it affects health and well-being at a global scale (part 4).
TL;DR: Vaccines work and save lives.

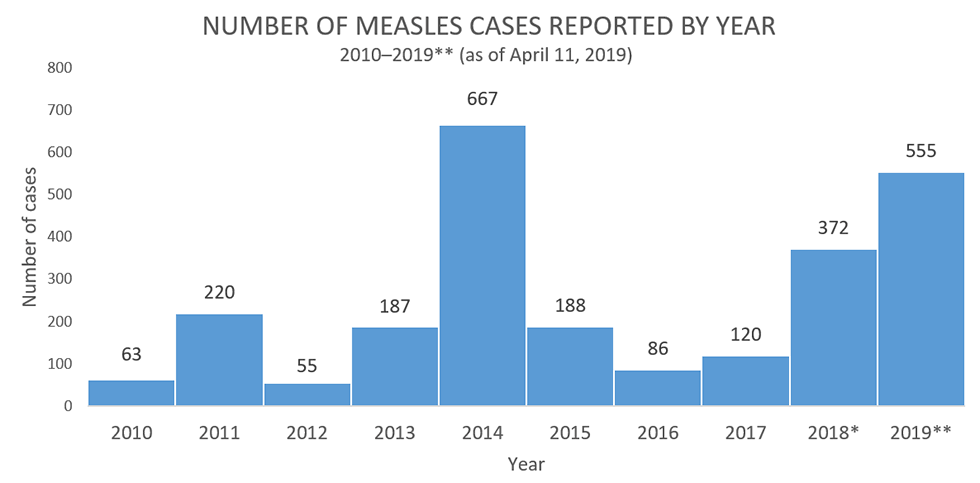
More recently in the news, we have heard about measles cases in the USA being at the second highest level in 25 years and with that number expected to rise. This statistic may surprise you given that measles was declared to be eliminated (absence of continuous disease transmission for greater than 12 months) in the USA in 2000. So why are we seeing a resurgence of late? The answer is simply because certain individuals are not being vaccinated before coming into contact with someone with the disease (usually when travelling abroad).
So why aren’t people getting vaccinated? A lot of this has to do with ignorance with respect to how vaccines work, although in some cases it is it is adherence to a belief system that is intractably resistant to fact and observation of reality. In light of the former, here’s a brief primer on vaccinations–there’s not much we can do for the latter, you see.
How do vaccines work?
Your immune system protects your body from pathogens (which cause disease). Pathogens are covered with tiny molecules called antigens. When your body detects one of these antigens, your immune system kicks into drive and mounts a response. If you are a healthy adult, most of the time, you will get sick and recover–although this is not always the case (for example, if you contract HIV). This also means that younger individuals with underdeveloped immune systems or older individuals with compromised immune systems may be at a much higher risk for the same infection.
A vaccine is like a pathogen imposter–it looks like the pathogen, triggering an immune response, but does not make you sick. There are four main types of vaccines, live attenuated, inactivated, subunit, and toxoid. When your body comes into contact with antigens on the vaccine, it produces antibodies specific to the pathogen’s antigens that the vaccine is mimicking. This primes your body to quickly respond to and neutralize the pathogen in the future, conferring immunity.
Some vaccinations, such as pertussis, require a “booster shot” subsequent to the initial vaccination. The reason a booster shot is needed is simply because the number of circulating antibodies for a given pathogen decreases over time. In highly contagious infections, having low levels of antibodies decreases the speed at which the body can respond to a pathogen–a booster shot eliminates this problem by increasing the overall level of circulating antibodies. It is therefore imperative that you stay current with recommended immunization schedules.
When a large percentage of the population is vaccinated against a disease, the spread of that disease is limited. That is because the disease has few targets to infect– most are protected and most won’t become infected and spread the disease. As a result, the larger population that is immunized indirectly protects those who aren’t vaccinated from the disease–a principle known as herd immunity. Depending on the contagiousness of the disease, the percentage of the population that is required to be vaccinated in order for herd immunity to be successful can vary–this is called the herd immunity threshold. Outbreaks, such as the one we are currently seeing in the USA, are a consequence of a large enough number of individuals within a specific population not being vaccinated and thus, an insufficient level to reach that herd immunity threshold. It is important to note that herd immunity relies on two assumptions: 1) that individuals in a population are randomly mixing and 2) that uniform immunity is achieved through vaccination. This simply means, if you live in a very small town in the state of New York, USA, where only 1% of the population is vaccinated against a disease, then chances are high you will get sick if you are unvaccinated and you come into contact with someone who gets that disease (and it is easily transmitted). This is true, even if, for example, the average vaccination rate in the state of New York or even in the entire USA is at the herd immunity threshold for that disease.
Fact: The herd immunity threshold for measles requires that 93-95% of the population be vaccinated.
How are vaccines mass produced?
Vaccines are made by first generating the antigen that induces the immune response we previously described. This includes growth and/or harvesting of the pathogen itself or generation of recombinant proteins from the pathogen. The pathogen is grown in different cell types, such as chicken embryos. Once the pathogen has replicated, the antigen is separated from the pathogen and then purified. Then, the vaccine may be strengthened by adding an adjuvant (which non specifically enhances immune responses) or by adding preservatives which prolong shelf life by preventing contamination. In the final step, all of these components are mixed uniformly and then packaged for distribution. Of course, this is after safety and efficacy has been established (see below).
Fact: Some people have argued that their religion prevents them from getting vaccinated because embryonic tissue is used in their generation. However, of the major religions in the USA only two religions expressly discourage vaccination–the Church of Christ, Scientist (whose adherents are known as “Christian Scientists”) and the Dutch Reformed Church.¹
¹https://www.historyofvaccines.org/content/blog/religion-vaccination-confusion
How is safety and efficacy evaluated?
All vaccines undergo extensive safety and efficacy testing in animals before they are even tried in humans — this is why severe reactions from the use of vaccines are 0.3% and lower. Researchers test candidate vaccines in cell cultures and in animals such as mice, rabbits, guinea pigs, or monkeys. If the vaccine appears promising in these preclinical experiments, it may go on to be carefully tested in people. Here, researchers must submit an Investigational New Drug (IND) application to FDA, and clinical trials begin–usually with a small group of humans. If all goes well, larger phases of testing will be conducted. Phase 1 trials usually contain about 20 humans, Phase 2 trials about 50 to ~300, while Phase 3 trials may involve thousands of humans. If there are no adverse effects, researchers may then apply to FDA for a license to market a vaccine–called a Biologics License Application (BLA). An expert advisory committee is convened weighing all of the pre-clinical and clinical safety and efficacy data and a vote taken on whether to approve the vaccination. If approved, the FDA continues to do follow-up surveillance to monitor safety, including inspection of the manufacturing facility, and random testing of vaccines for potency, safety and purity for as long as that vaccination is manufactured.
Fact: Vaccines save the lives of non-human animals too!

In our next piece, we will describe how misinformation and lies rapidly spread to produce the “anti-vaxxer” crisis that we are in today.
