
May 15th 2020
I often think that many human therapies developed with animal research must follow a linear or step-wise trajectory. First, there’s a significant medical issue that burdens the welfare of humans and/or the economy. Or, there’s some aspect of biology that we don’t yet understand enough. Then, we determine that it would be worthwhile to study this issue or aspect of biology further to benefit human welfare, the economy, or scientific knowledge. After extensive research, spanning multiple decades, we gather enough knowledge to translate animal research into a therapy for humans. And voila! It’s called a breakthrough! Thank goodness for animal research! But, as I’ve learned over the years, that’s not really how science works. A more realistic example of animal research to human therapy trajectories comes from the field of ‘open fetal surgery’ to correct a malformation of the neural tube, referred to as spina bifida.
Spina bifida
Our spinal cord acts like a switchboard, relaying messages to and from the brain and body. Damage to the spinal cord results in paralysis, interfering in the messaging between the spinal cord and the brain. Many people are familiar with ‘Superman’ star Christopher Reeves, who suffered major spinal cord damage following a horseback riding accident that paralyzed him from the neck down. Such damage is tragic and the topic of extensive scientific investigation. But damage does not always come from traumatic injury.

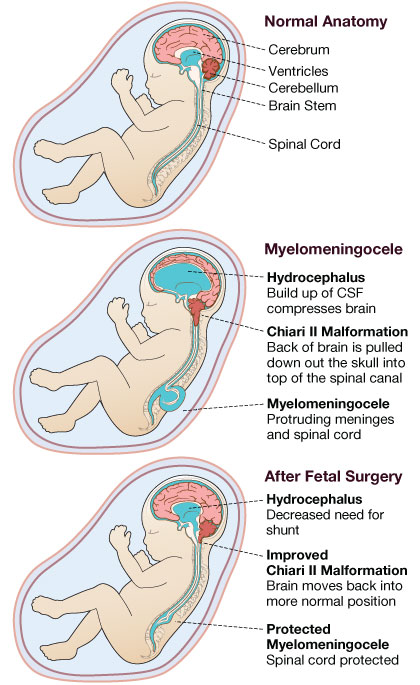
Each year in the United States, more than 1,000 babies are born with spinal cord damage through a condition called spina bifida, or split-spine. In one of the most serious types of spina bifida, the lower spinal cord, filled with cerebrospinal fluid, appears to protrude out of the baby’s lower back. This condition is also associated with hydrocephalus, paraplegia, incontinence, multiple orthopedic pathologies, and endocrinologic, sexual, intellectual, and psychosocial abnormalities. It is also significantly associated with a Chiari II malformation (~95%) where a portion of the cerebellum of the brain extends out of the skull and into the spinal cord region. This causes severe problems with the neck and swallowing, and requires surgery in the back of the head to make room for the protrusion.
There are many ways to deal with spina bifida. Supplementing the mother’s prenatal diet with folate is the leading preventative measure in terms of public health to lower the incidence of the condition. In terms of treatment, the most common method is to operate on newborn babies, postnatally, by surgically coaxing the spinal cord to its proper place along the spinal vertebra, draining the spinal fluid, and closing the open defect. Doctors also insert a permanent shunt near the spine to drain fluid throughout the child’s life. This surgery prevents further damage to the nervous system like hydrocephalus, prevents infections like meningitis, and removes the pain associated with the condition. However, it often does not allow for recovery of motor or bladder control.
Over the past decade, operating on the fetus before the mother gives birth has become more commonplace, thanks to extensive years of animal research and clinical trials. This surgery provides great benefit, further preventing damage to the nervous system like hydrocephalus, the associated neurological dysfunctions, and negating the need for a permanent shunt to drain the fluid that can build up over the child’s life.
Families and patients suffering from spina bifida largely have animal research to thank for new practices involving ‘open fetal surgery’ and general treatment of spina bifida. But as you will see, human therapies are not always perfect and the apparent benefit described by animal experiments often excites society to move forward with clinical practices, sometimes without regard as to whether additional animal experiments may be needed.
Spina bifida is reversible
For a large chunk of our history, scientists and clinicians alike largely believed the malformation of spina bifida (that opening in the neural tube, exposing the spinal cord) directly caused the symptoms of hydrocephalus, paraplegia, neurological dysfunction, incontinence, etc. However, convincing research on other congenital malformations (i.e. congenital hydronephrosis) began to suggest that the damage associated with the malformation worsens throughout fetal development. Scientists and clinicians often refer to this as a two-hit injury. First, there is a congenital malformation. Then, second, that malformation leads to increasing damage the longer the fetus remains within the mother.
This realization of a two-hit process intrigued a group of scientists, in the early 1990s, to see if this held true for spina bifida. So, they studied a number of human fetuses with spina bifida across different time points in pregnancy (i.e. gestation). They discovered the two-hit process was likely true for spina bifida. Early stage fetuses appeared to have less spinal cord damage than later stage fetuses. This indicated that the malformation exposed the nerve tissue, allowing amniotic fluid to come into contact with the spinal cord and cause damage. The longer the spinal cord was exposed the more damaged it became. Expectedly, this quickly inspired many to start developing methods for addressing the malformation as early as possible. Albeit, many people with friends and family suffering from the disease had urged doctors to consider such surgeries back in 1972.
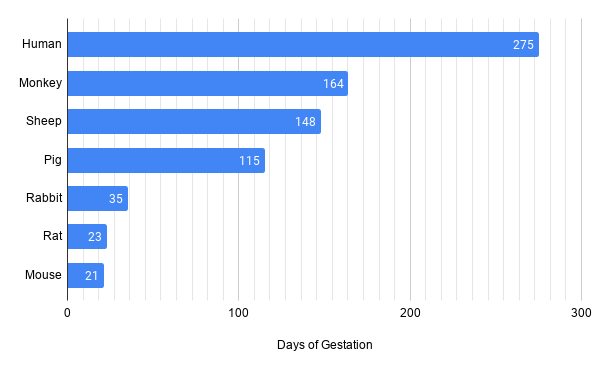
So, in the early 1990s many animal experiments on spina bifida and ‘open fetal surgery’ began to take place. First, scientists needed to verify whether just exposing the fetal spinal cord to the amniotic fluid caused damage. Across the world, a number of animal models were quickly developed using monkeys, rats, pigs, rabbits, and sheep. Here, scientists operated on pregnant dams and made small incisions in the lower spine region of the fetuses to surgically induce an artificial form of spina bifida. Now, developing this test was no easy task. Scientists had to operate on pregnant dams to make an opening on the back of the fetus that exposed the spinal cord, then stitch the dams back up, and wait until the day of delivery. Lots of differences in biology also have to be considered, mainly the time of gestation or the time the spinal cord is exposed to amniotic fluid.
Experiments on sheep in 1995 were the most convincing since the surgery caused newborn lambs to be born paraplegic and incontinent — classic symptoms attributed to spina bifida. Such experiments also determined that surgical repair of the ‘spina bifida model’ (just exposure of the fetal spinal cord to the amniotic environment) 4 weeks after spinal cord exposure, resulted in newborns that were neurologically normal. But the ultimate proof didn’t come until 2007 from a genetic mouse model of spina bifida, resulting in 34% of pups to be born with spina bifida without the need for the artificial spina bifida model used in the monkey, rat, pig, rabbit, and sheep models. Investigation into the anatomy of the spinal cord in early gestation showed no difference between control pups and spina bifida pups. But upon birth, pups were paralyzed and had minimal spinal cord remnants. This study definitively showed that the two-hit injury process occurs in spina bifida.
Fetal surgery in humans
The first fetal surgeries for spina bifida in humans were done in 1997 and 1998 at Vanderbilt University and Children’s Hospital of Philadelphia, respectively. For the few fetuses, they found that the surgery reduced the need for a shunt by 50% and there was favorable development of the head, brainstem function, motor function of legs, and several neurodevelopmental parameters. Unfortunately, the repair did not have any positive effects on incontinence. This initial evidence led to a larger trial to be undertaken in 2003. By 2010, after testing 183 pregnancies, across three hospitals, researchers determined that the evidence for benefit was so overwhelming that they needed to halt the trial and only conduct open fetal surgery. Just like the earlier studies, the newborns who received fetal surgery had fewer needs for a shunt and superior mental and motor development at 30 months of age compared to those who received postnatal surgery for spina bifida.
However, some spina bifida experts claimed the results from this study revealed that open fetal surgeries are problematic and more research is necessary before widespread implementation. First, the surgery itself requires a great deal of skill and training for surgeons and hospital staff, usually requiring 35 surgeries before competence is reached. In cases with low competence, a subsequent postnatal surgery is needed in addition to the prenatal surgery to correct the imperfection.
Second, open fetal surgery often leads to premature birth at around 34 weeks (46% of babies) instead of 40 weeks gestation typical to humans, or the 38 week gestation typical of babies with spina bifida and given postnatal surgery (85%). Although our medical system is getting better at treating preterm birth, it still has inherent risks like respiratory distress syndrome, which is a breathing disorder from immature lungs. Thus, fetal surgery may decrease mental and motor development issues associated with spina bifida, but also increases additional disabilities like respiratory distress syndrome.
Third, fetal surgery shows little to no improvement regarding the Chiari II malformation in the brain, and thus requires additional postnatal surgery to make room for the extended portion of the cerebellum. Given these complications and the increased training necessary some hospitals have chosen to abandon the practice despite the benefit and are awaiting new procedures that are less risky and more effective.

Wrap-up
In summary, it’s clear that animal research for treating spina bifida should continue despite the open fetal surgery treatment. You might hear claims that ‘open fetal surgery’ is ethically necessary and lifesaving but it comes with risks and does not address all symptoms associated with spina bifida (the Chiari II malformation).
This necessity for additional animal work despite a successful therapy makes sense. Around 32 years ago an experiment with sheep indicated that open fetal surgery may be beneficial for treating spina bifida. Just 2 years later, the first open fetal surgery on humans was a success. But it took 20 years, in 2010, for a randomized clinical trial across 3 hospitals to suggest it was worthwhile. While the randomized trial was running, a mouse study in 2007, showed ultimate evidence for the logic behind the surgery suggested by the sheep experiment back in 1988. Due to the extensive training necessary for the surgery, increased risk for preterm delivery, and neglect for the Chiari II malformation, animal research for treating spina bifida continues. For example, stem cell therapies involving the injection of mesenchymal stem cells are being experimented with rabbits, and non-invasive intra-amniotic therapies are being experimented with rats. So, despite a therapy (‘open fetal surgery’), animal research continues.
Justin Varholick, PhD
The author is a biomedical scientist currently studying how the environment can interfere with the healing process after injury.
Further reading
Yale New Haven Hospital team performs surgery on unborn baby
Fetal surgery for myelomeningocele is effective: a critical look at the whys
Fetal surgery for spina bifida
