
April 26th 2021; Updated August 19th 2021
Allyson J. Bennett, Sangy Panicker, Amanda Dettmer & Jeremy D. Bailoo
In our previous post, we provided descriptions of how and why vaccines work and detailed how safety and efficacy are evaluated for the lifetime of any vaccine that is in use. In this piece we delve into the various COVID-19 vaccines currently approved for use around the world. We also remind readers that worldwide vaccination access and delivery varies greatly, with tragic consequences.
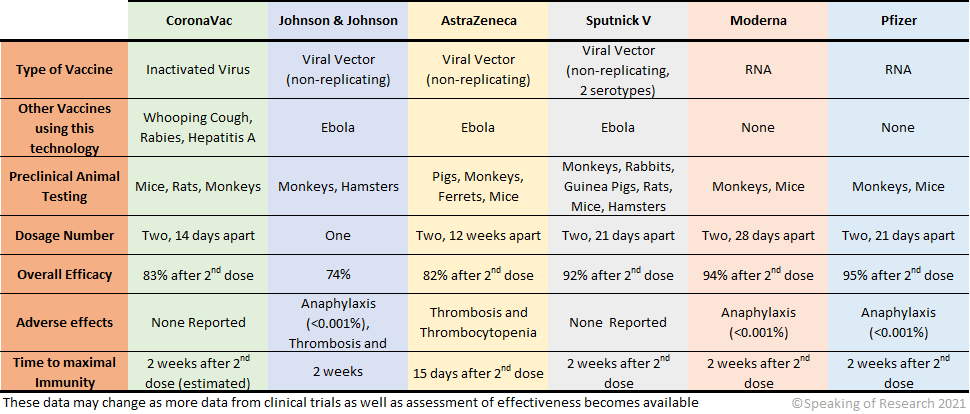
Vaccines currently approved for use by the World Health Organization (WHO) are Pfizer-BioNTech, SK BIO AstraZeneca, Janssen (Johnson & Johnson). The Moderna vaccine is approved in the US, Gamaleya’s Sputnik V is approved in 62 countries, and Sinovac’s CoronaVac is approved in 22 countries. The Serum Institute of India (COVISHIELD), which is also approved by the WHO, is the AstraZeneca vaccine, manufactured in India. This list is not exhaustive, but rather represents the vaccines that are most prevalently used globally.

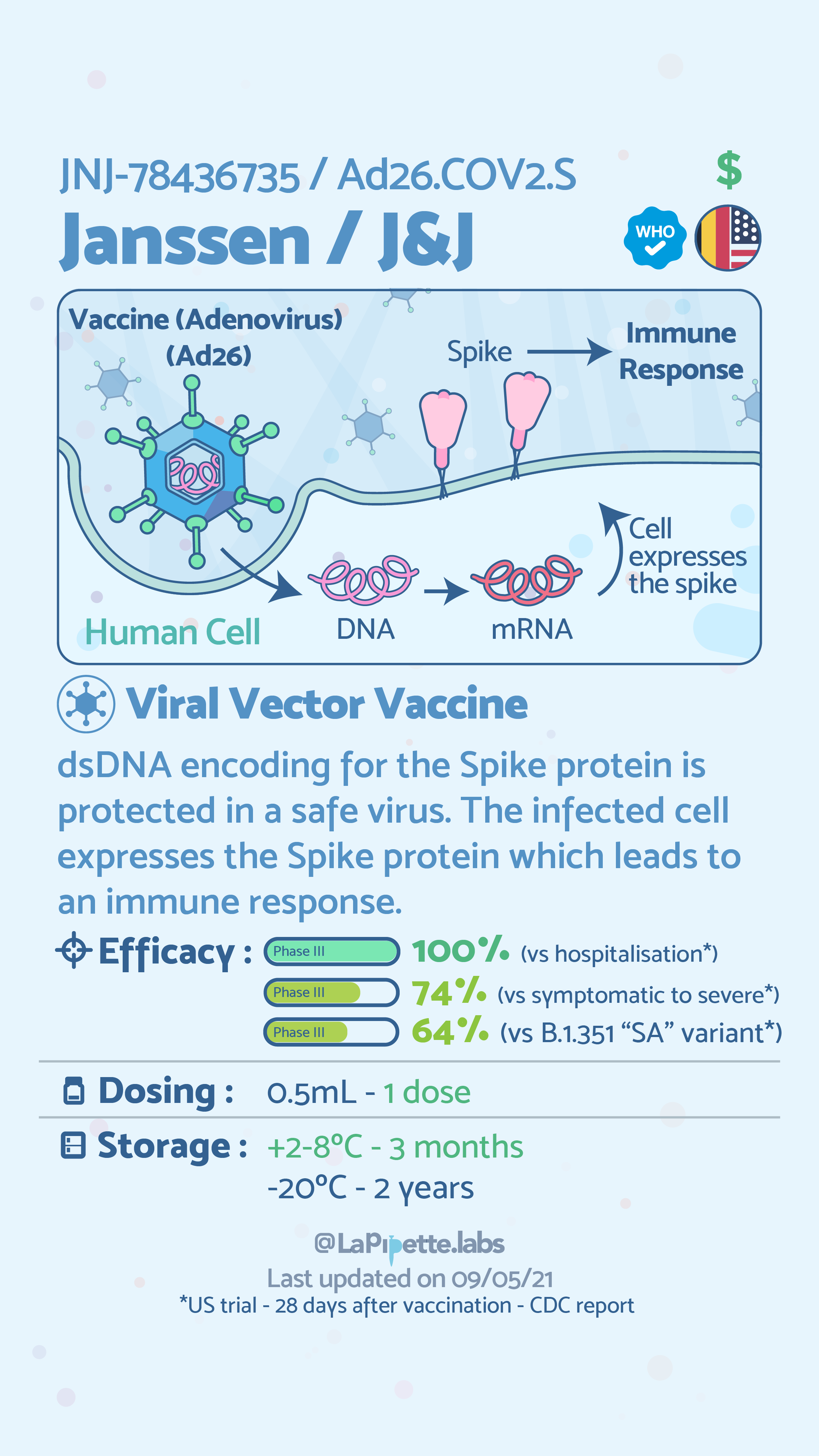
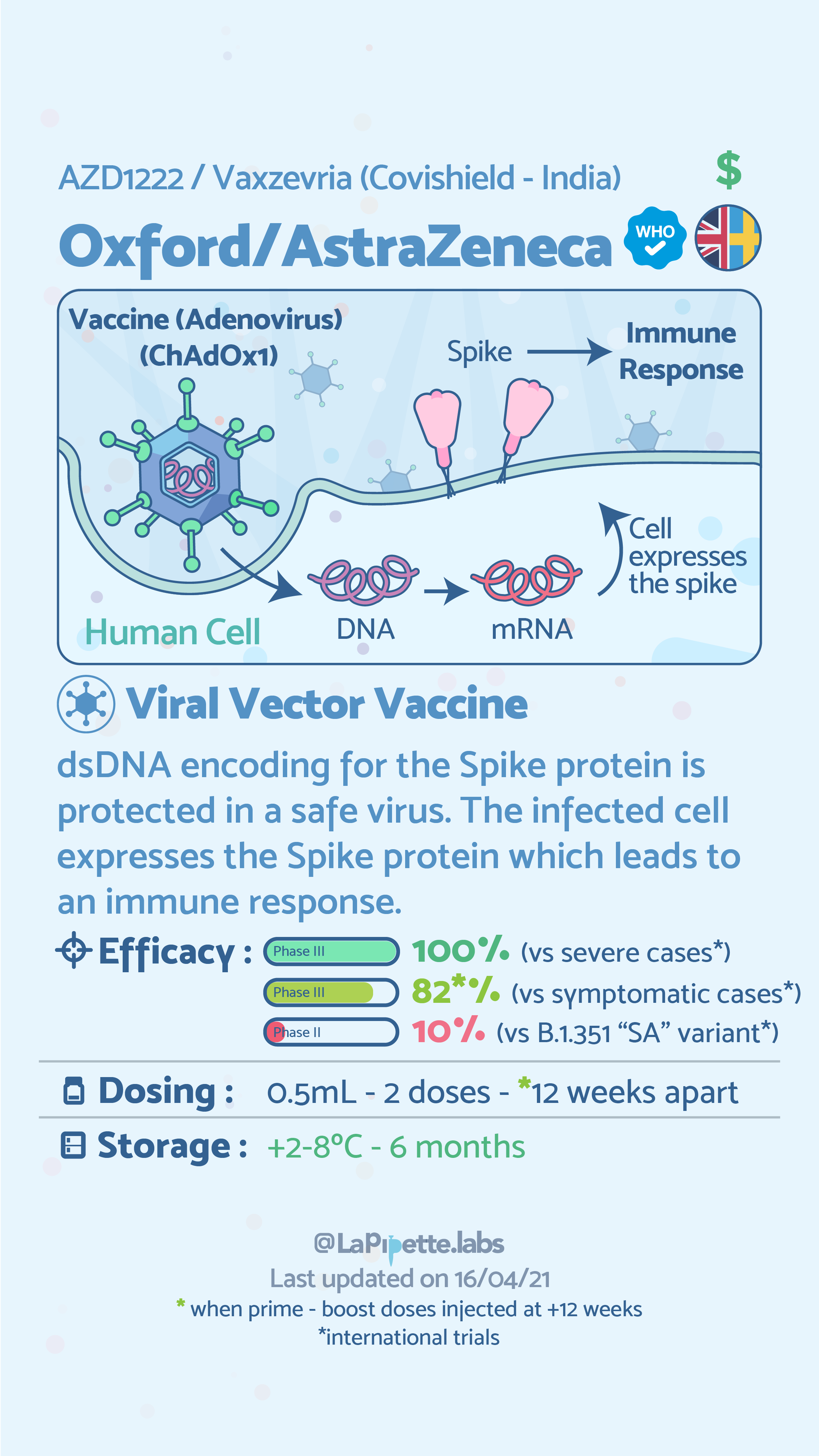
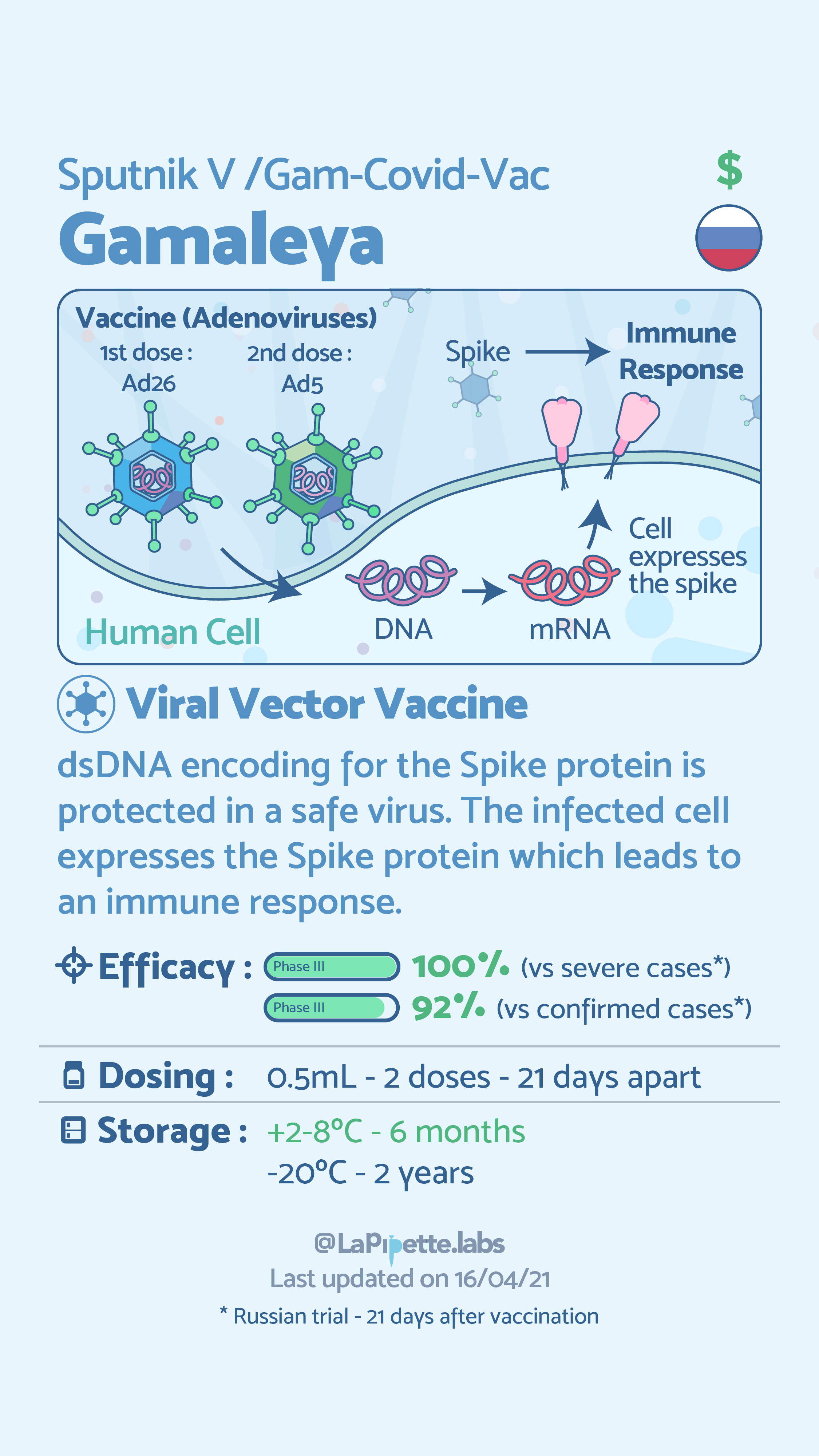
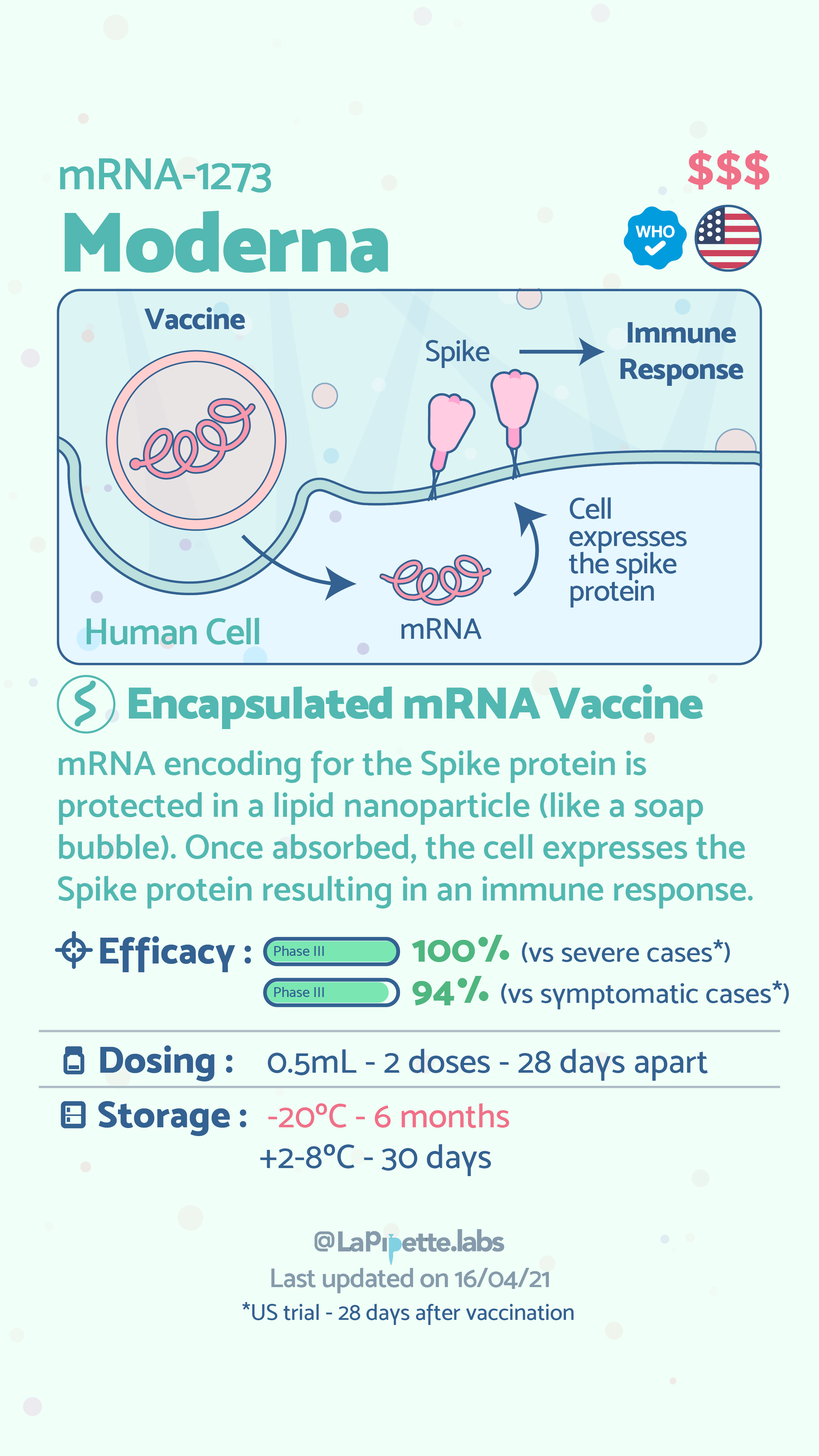
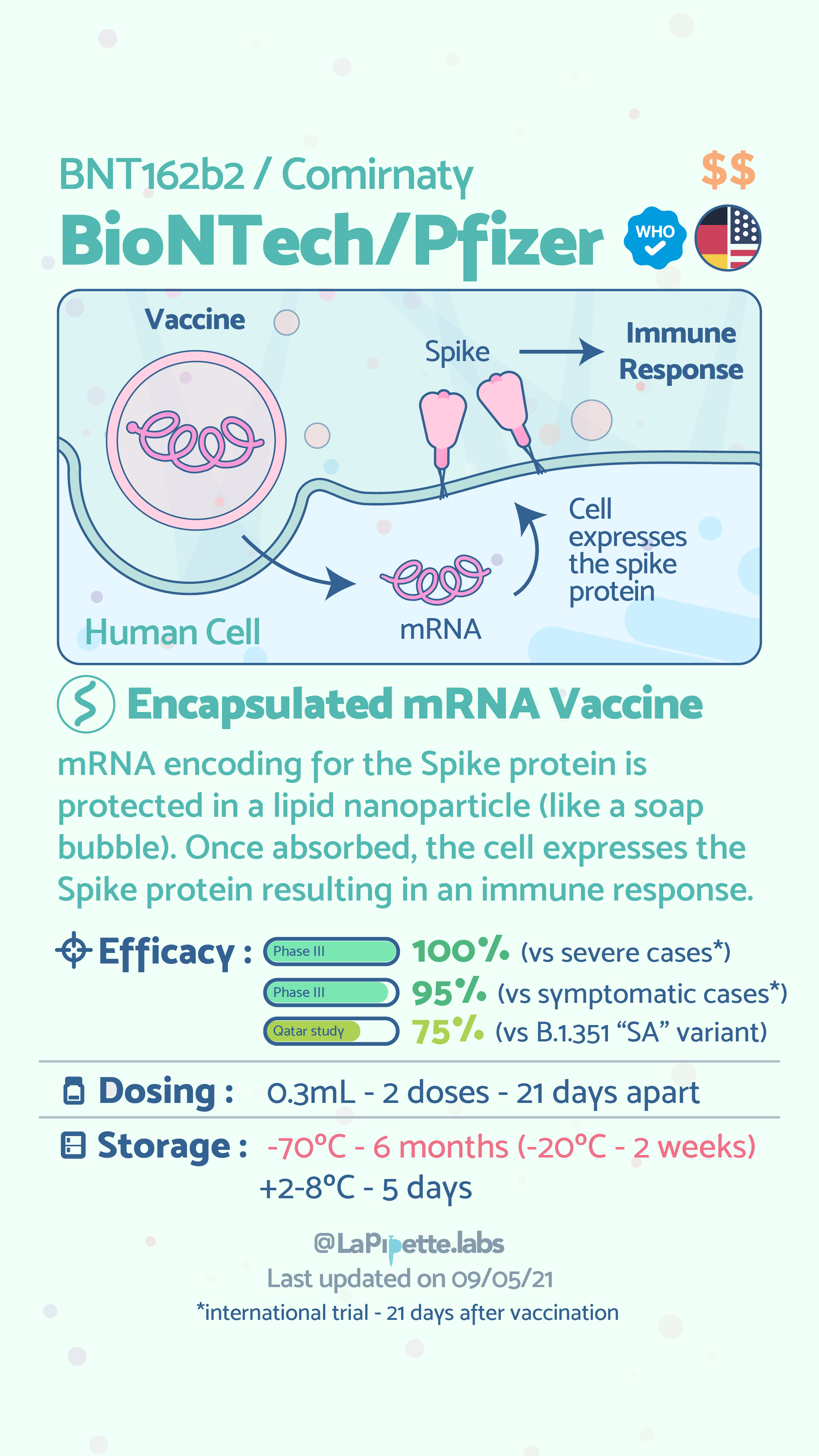
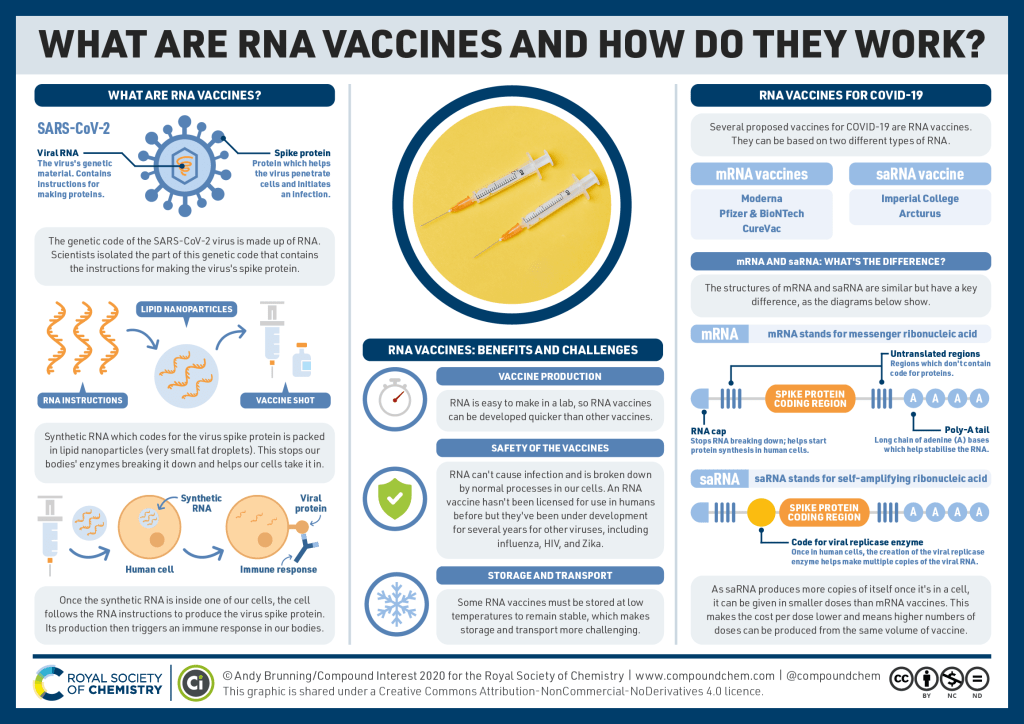
As can be seen above the common vaccines for COVID-19, currently use three of the six types of vaccine technologies. Globally, however, there are over 180 vaccines and therapeutics being evaluated in preclinical trials for COVID-19, some of which use the remaining three technologies. The general principle of all of these vaccines, and vaccines in general is to expose an individual to a harmless version of the whole virus (inactivated virus) or a piece of the virus—in the case of COVID-19, the spike protein. The exposure allows the body to identify the foreign element (pathogen) and prompts the immune system to create antibodies to that pathogen. The antibodies neutralize the virus and protect the individual from future infection. The following infographics provide further description of how viral vector and RNA vaccine technologies work.

The role of basic research and preclinical and clinical trials in safety and efficacy testing.
As we wrote about at the start of the pandemic, our ability to produce a vaccine within a year—was possible because the amazing accomplishment depended on decades of previous discoveries. It depended on over a decade of #AnimalResearch into coronaviruses, such as Severe Acute Respiratory Syndrome (SARS) and the Middle East Respiratory Syndrome (MERS), along with decades of prior research into mRNA vaccines. As we highlight in the table above, the pre-clinical research evaluating safety and efficacy prior to human use was performed with many species of animals.
Fact: Those opposed to animal research continue to de-emphasize the valuable role that basic research as well as applied research with animals has played in our response to the pandemic.
#FactCheckNeeded #MadePossiblebyAnimalResearch #MPAR.
But what does safety and efficacy really mean? For individuals making choices about whether to take a vaccine, these are key questions. Both terms are used in a very specific sense both pre-clinically (before humans are tested) as well as clinically (when humans volunteer for tests). Pre-clinical and clinical testing, as we highlighted in our previous piece, are two of the many lines of defense that our system of oversight uses to establish that a drug works (efficacy) and that it does not lead to bad outcomes in humans (safety). Notably, this does not mean that all bad outcomes can be predicted or stopped prior to approval for widespread use. The tests do provide us with a reasonable amount of confidence that once a drug, like a vaccine, is tested in humans really bad things don’t happen to a great number of people. Given that individuals can vary from each other in many ways—race, gender, pre-existing health conditions, etc.—it is not always possible to represent all of these factors within a clinical trial. Some of the factors which are associated with adverse effects in people will only become obvious when the drug is approved and is being used widely. Continued monitoring after the drug or vaccine is taken by a large number of people also can expose safety concerns for subsets of individuals. The continued evaluation of efficacy after clinical trials are concluded and when the drug is approved for use in humans is termed effectiveness.
Fact: Both safety and effectiveness assessment is performed for any drug approved for use in humans for the life of that drug.
A number of outcomes are measured to assess whether, and how well, COVID-19 vaccines work, or their efficacy. While we think about good outcomes in terms of preventing COVID-19 infection and prevention of severe COVID-19 (which involves hospitalization and sometimes death) the development of neutralizing antibodies to COVID-19 is also important. In terms of the vaccines approved for use in the US and globally, efficacy is high for most vaccines—between 85-100%. What is also true though is that no vaccine almost certainly results in a higher risk of contracting COVID. There are also other factors which affect our ability to compare the different vaccines. For example, the clinical trials of Pfizer and Moderna tested for any symptomatic COVID-19 infection while Johnson and Johnson evaluated protection against severe COVID. A host of other factors (highlighted in the video below) also make direct comparison of efficacy between vaccines quite difficult.
Fact: Despite having different efficacy rates, interim analyses highlight that the common vaccines administered in the US for COVID-19 are successful at preventing severe COVID—with rates between 85-100%. This means that while it may still be possible to get COVID, the risk of dying from COVID-19 decreases dramatically after vaccination.
What about the safety of COVID-19 vaccines? Vaccines currently approved by the US and/or WHO (Pfizer-BioNTech, SK BIO AstraZeneca, Janssen/Johnson & Johnson, Moderna) have common side effects that may be experienced. Similar to the seasonal flu vaccine, these side effects include injection site pain, headaches, fatigue, muscle pain—with symptoms often being worse after the second dose (for two dose vaccines). These effects are usually acute, lasting only a few days.
Both AstraZeneca and Johnson & Johnson paused vaccine rollouts after reports of thrombosis (blood clots) and thrombocytopenia (low platelet count), while earlier on, anaphylaxis (allergic shock) was reported with Moderna, Pfizer, and (later) Johnson & Johnson vaccines. As a consequence of the early reports of anaphylaxis, the CDC updated its guidelines to further ensure the safety of those receiving the vaccine. For both the AstraZeneca and Johnson & Johnson vaccines, an abundance of caution was exercised with respect to blood clots and low platelet count.Trials were paused and data were carefully examined. It is important to note that trials were paused even though the base rate—the incidence of blood clots and low platelet count that occur in the population regardless of vaccination—was far lower than that associated with the vaccine. It is also important to note that even though two things co-occur, this does not mean that they cause one another. Finally, it must be noted that clinical trials cannot include the entire population and all of the different factors and conditions that vary between people and that might affect response to a vaccine.
Fact: Thus far, the US CDC and the European Medicines Agency have given permission for AstraZeneca and Johnson & Johnson to be administered. Their advice rests on three considerations. 1. the fact that the incidence of blood clots (thrombosis) and low platelet count (thrombocytopenia) following vaccination are extremely rare. 2. that there is no evidence that the vaccine causes these adverse outcomes. 3. The risk of severe health consequences, including death, from COVID-19 infection is high.
Should I get vaccinated? Which vaccine should I take?
As we have continually highlighted at Speaking of Research—facts matter.
The facts demonstrate that COVID-19 vaccines dramatically reduce the incidence of severe COVID-19 and thus saves lives.
The data also suggests that the common vaccines approved in the US, for example, perform well in preventing infection from the common COVID-19 variant, B.1.1.7. As long as we have individuals that continue to refuse to be vaccinated, then the chance of seeing further variants that are perhaps more virulent will increase. This means that the pandemic will drag on and life under COVID-19 may become our new normal.

In our next two pieces, we will revisit the Andrew-Wakefield Scandal and highlight how his actions precipitated the anti-vaxxer crisis that persists today.
