
Today scientists at the Newcastle University Movement Laboratory announced that they have succeeded in restoring the ability to grasp and pull a lever with a paralysed hand using spinal cord stimulation. In a study undertaken in macaque monkeys they demonstrated for the first time that it is possible to restore voluntary movement in upper limb paralysis and tetraplegia, where there has been damage to the upper regions of the spinal cord that blocks the nerve pathways which pass messages to the muscles from the brain.

At this point some of you are probably thinking ‘Wait a minute, didn’t you just write about spinal stimulation being used to restore voluntary movement in paralysed human patients, why is this news?’ Well, it’s news because while both techniques use electrical stimulation they use it in very different ways, and will benefit paralysis patients in different ways.
In the study we discussed earlier this month Professor V. Reggie Edgerton and colleagues restored voluntary movement to the legs of 4 paraplegic men by using epidural stimulation to excite spinal nerve networks below the injury in a diffuse way. The method exploits the fact that spinal nerve networks are to some degree, “smart.” If certain sensory information is provided, for example pressure on a foot, the activated spinal cord can recognize this information and respond by generating a specific pattern of muscle activity, without requiring input from the brain. This activity can be enhanced with repetition and training, and also takes advantage of the fact that often even in spinal injuries that appear to be complete not all the nerve connections through the area of damage are broken, so once the network below the injury is activated these remaining nerve connections can be exploited to achieve conscious control over movement. However, epidural stimulation may not restore voluntary movement in spinal patients with most complete injuries, and it is not clear that the degree of voluntary control restored will be enough to allow all the patients treated so far to walk unaided.
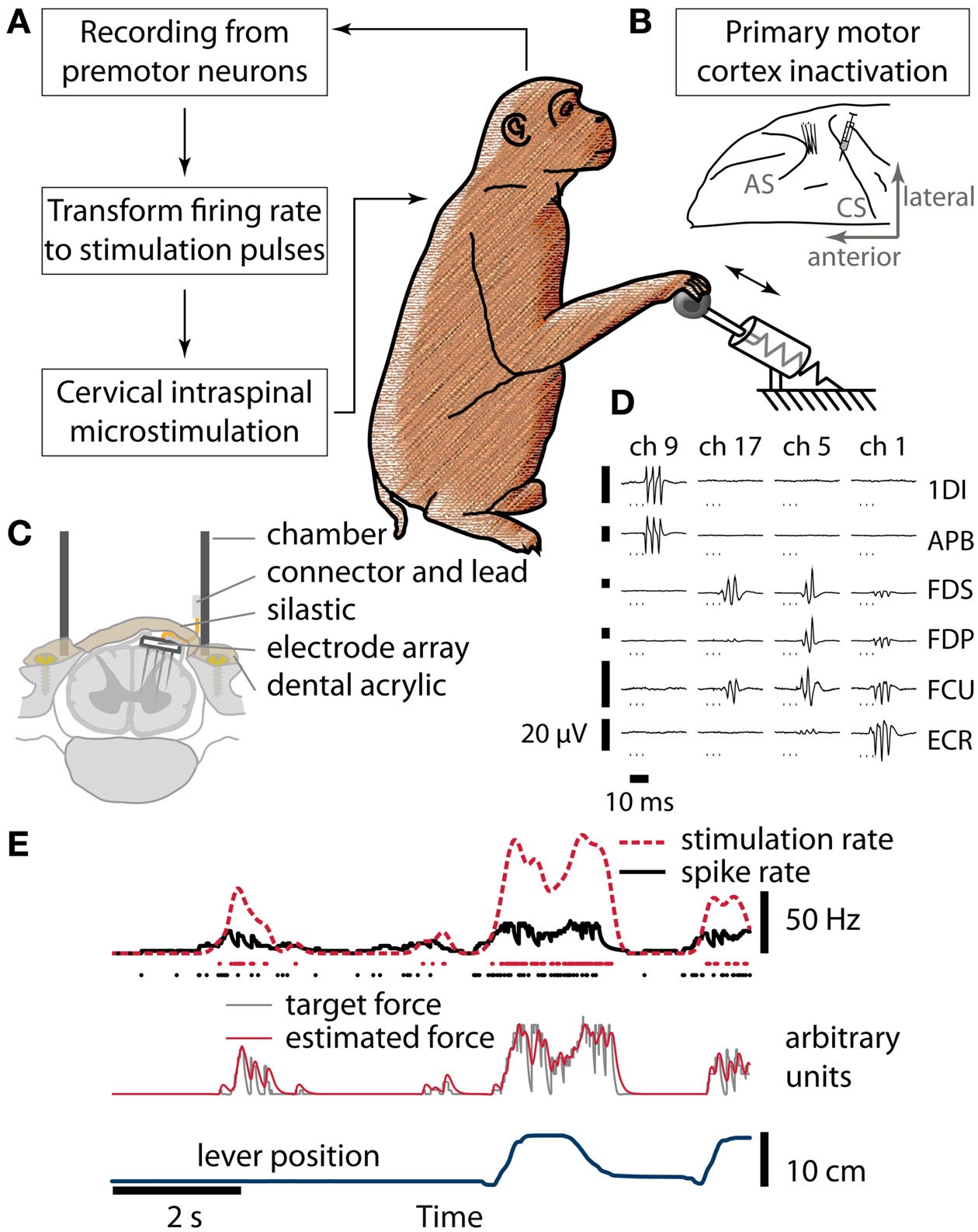
Intraspinal microstimulation, the technique pioneered by the Newcastle University team led by Dr Andrew Jackson and Dr Jonas Zimmermann is very different. Rather than stimulating the spinal cord in a diffuse manner to increase activity in a non-specific way, it works by transmitting signals from the brain to specific spinal nerve circuits below the injury, in order to activate particular muscle groups (1). Working with macaque monkeys, they recorded the activity of individual nerve cells in the premotor cortex of the brain using a microwire array (similar to the brain machine interfaces used to control robot arms), processed those signals in the computer, and then used the output from the computer to stimulate specific motor neuron circuits in the spinal cord via an implanted microelectrode array that in turn control the movement of the hand.
Intraspinal microstimulation does involve more invasive surgery than epidural stimulation, but opens up the possibility of new treatments within the next few years which could help stroke victims and upper spinal cord injuries to regain some movement in their arms and hands. Intraspinal microstimulation may also benefit patients whose lower spinal injuries are too complete for epidural stimulation to enable them to walk, and provide them with a much finer degree of control over movement that could mean the difference between being able to move their legs and being able to walk fluidly.
To conduct this study, published today in the journal Frontiers in Neuroscience, the team first trained macaque monkeys to grasp and pull a spring-loaded handle in order to obtain a treat such as a piece of dried fruit or yoghurt. The monkeys were then temporarily paralysed, using a drug that wore off after about two hours. During that time the monkey had no movement in their hand and was unable to grasp, even though most of the brain was functioning normally. But when the stimulation circuit was switched on the monkey was able to control its own arm and pull the handle.
This is an advance that rests on decades of basic research to understand the pathways within the nervous system and applied research to develop the technology required to restore function, undertaken by thousands of scientists around the world. The microwire array used to record single neuron activity in the brain was developed through studies in macaques by the Newcastle team in 2007, while more recently they undertook a series of studies which examined different patterns of microarray electrostimulation of motor neurons in the upper spinal cord to identify those that could restore voluntary movement.
Commenting on their research Dr Zimmermann noted that:
“Animal studies such as ours are necessary to demonstrate the feasibility and safety of procedures before they can be tried in human patients, to minimise risk and maximise chance of successful outcomes.”
The next stage will be to further develop the technology to eventually have a small implant for use in patients that can then form the link between the brain and the muscles, and Dr Jackson is optimistic that this technology will be available to patients within a few years
“Much of the technology we used for this is already being used separately in patients today, and has been proven to work. We just needed to bring it all together.
“I think within five years we could have an implant which is ready for people. And what is exciting about this technology is that it would not just be useful for people with spinal injuries but also people who have suffered from a stroke and have impaired movement due to that. There are some technical challenges which we have to overcome, as there is with any new technology, but we are making good progress.”
It’s tempting to think of intraspinal microstimulation and epidural stimulation as competing techniques, but this would be a mistake as it very likely that both will be used, separately or together, depending on the nature of an individual patient’s injury. The greatest benefits for patients may be achieved when these neurostimulation techniques are combined with other approaches such as regenerative medicine/cell therapy and active rehabilitation. In 2012 Jackson and Zimmerman published a review of neural interfaces in restoring movement which examined the evidence from both animal and clinical studies, which highlighted a process known as Hebbian plasticity which can be summarised as “cells that fire together wire together”. Evidence is mounting that stimulation of the spinal cord below the site of injury does not only bypass lost nerve pathways or awaken dormant neural networks, but actually promotes the development of connections between nerves on each side of the damaged area to create new pathways along which signals can be passed from the brain to muscles in the arms or legs.
Today we congratulate Andrew Jackson and Jonas Zimmermann – and the Wellcome Trust who funded their work – on their outstanding accomplishment, but we also remember that it is not happening in isolation. The true importance of the therapy published today that it is part of a neuroscience-driven revolution that will in a few years time begin to transform the lives of many thousands of people with spinal injury. We may not be there yet, but the destination is at last in sight.
Paul Browne
- Zimmermann J.B. and Jackson A.”Closed-loop control of spinal cord stimulation to restore hand function after paralysis” Frontiers in Neuroscience, Published Online 19 May 2014.
Addendum 21st May 2014: Interesting to note the comment by the animal rights group the BUAV that “Claiming, as do some apologists for animal research, that this news is worthwhile because the electrical stimulation in the monkeys ‘was used differently’ is desperate, and overlooks the importance of human-based studies and the contribution they have made.” which only shows that their ignorance (or willingness to lie about) this subject. The BUAV article also includes the usual outlandish claims about the monkeys used in this study being terrified, deprived of food and water etc. completely missing the point that this study required the active alert participation of the monkeys, so they needed to be relaxed and cooperative throughout it.
All surgery was accompanied by appropriate anesthesia and pain relief so that the monkeys would not suffer, and the monkeys used in this study were trained over a period of time through positive-reinforcement to gradually accustom them to the test apparatus used so that it caused them no distress. The monkey’s access to water was not limited, and their access to food in the study was only restricted for a few hours so that they were not too full to be interested in the food reward. While there is no doubt that this was an invasive procedure (just as the procedure will be for human patients) the BUAV’s comments completely misrepresented it.
To learn more about the role of animal research in advancing human and veterinary medicine, and the threat posed to this progress by the animal rights lobby, follow us on Facebook or Twitter.

Can I simply say what a comfort to find someone who really
knows what they are talking about on the net. You definitely know how to bring a problem
to light and make it important. More and more people need
to look at this and understand this side of the story.
I was surprised that you are not more popular since you
definitely have the gift.
Hello, im very impressed let me tell you more about my case im a 27 years old girl i had a car accident in 2005 i got my back bone broken and spinal cord injury in the T12 i was totally paralyzed for like 2 years had a couple of surgeries to fix my back and remove the compression and i got much better i worked really hard and had a lot of physic therapy and now i got much better i can walk on crutches but still i dont have any sensation or movability in my feet my problem is s1s2 L3L4 i was wondering if u could help me and if it my case can get any kind of progress if yes plz tell me how can i contact u and what exactly is needed to be done and im ready to come and do the surgery as soon as possible thanku soo much
i have a lazy eye
Do you think that will works with me ?
all the doctors who visited them said : no tratment :(